In-Silico Modeling of Blown-Out Myotomy (BOM)
Background
Laparoscopic Heller Myotomy (LHM)
LHM is performed either with an instrument called a harmonic scalpel or with simple blunt dissection using two laparoscopic graspers directed in opposite directions to stretch and tear the circular muscle fibers. The figures show the distal part of the esophagus being operated on. The top of the figures shows the diaphragm surrounding the esophagus. The LM are separated out and the CM are broken. The myotomy region takes the form of an ellipse.
Study Overview
Background
In this study, we used in-silico models to investigate of the impact of the shape and size of laparoscopic Heller myotomy (LHM), and the strength of the lower esophageal sphincter (LES) (due to the combined influence of LES tone and fundoplication) in the formation of blown-out myotomy (BOM).
Methods
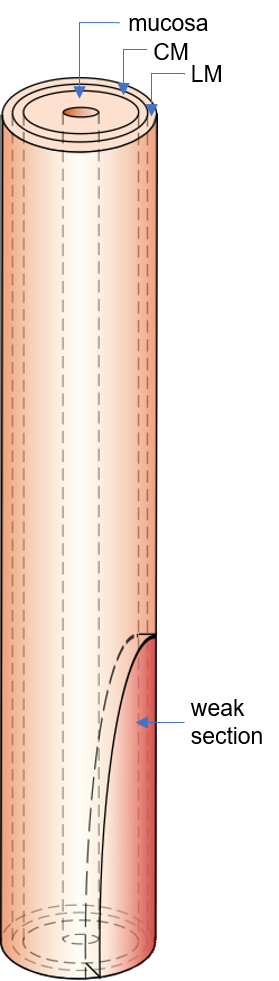
We performed three sets of simulations with an in-silico esophagus model with the LHM influenced region modeled as an elliptical section devoid of muscle fibers. The first, second and third set of simulations investigated the effect of the shape and size of LHM, the different types of contractions, and the role LES, respectively on the formation of BOM.
Results
The first simulation set showed that both increasing and decreasing the maximum length of LHM from a reference value (major axis: 60 mm, minor axis: 7mm) improved BOM, while decreasing the width seemed to minimize the extent of BOM. The second simulation set showed that that peristalsis leads to the most pronounced BOM, followed by pan-esophageal pressurization and spasms. The third simulation set shows that with the presence of an LES tone, a normal esophagus was able to empty the bolus, but the weakened section of the esophagus formed a BOM even without the presence of an LES tone.