Presenting Author:
Nao Souma, M.D.
Principal Investigator:
Tamara Isakova, M.D.
Department:
Medicine
Keywords:
FGF23, mineral metabolite, living kidney donor, nephrectomy, glomerular filtration rate
Location:
Ryan Family Atrium, Robert H. Lurie Medical Research Center
C48 - Clinical
Fibroblast growth factor 23 and mineral metabolites following kidney donation
Fibroblast growth factor 23 (FGF23) is an endocrine hormone that regulates phosphate and vitamin D homeostasis. It is secreted from osteocytes as either full-length intact FGF23 or C-terminal FGF23 fragments. Levels of FGF23 rise in patients with chronic kidney disease (CKD), and elevated FGF23 is independently associated with increased risks of cardiovascular disease events and mortality. Other mineral metabolite disorders, including calcitriol deficiency, secondary hyperparathyroidism, hyperphosphatemia, and hypocalcemia are common complications of kidney failure. However, it is not clear how levels of these mineral metabolites are regulated early in the course of CKD, when the glomerular filtration rate (GFR) first begins to decline.
We enrolled 34 living kidney donors (mean age 40 ± 13 years) who underwent nephrectomy during 2010-2011. We measured serum creatinine, phosphate, calcium, parathyroid hormone (PTH), and FGF23 before and 1, 2, 14, 180, and 365 days following donation to examine mineral metabolite changes before and after donation.
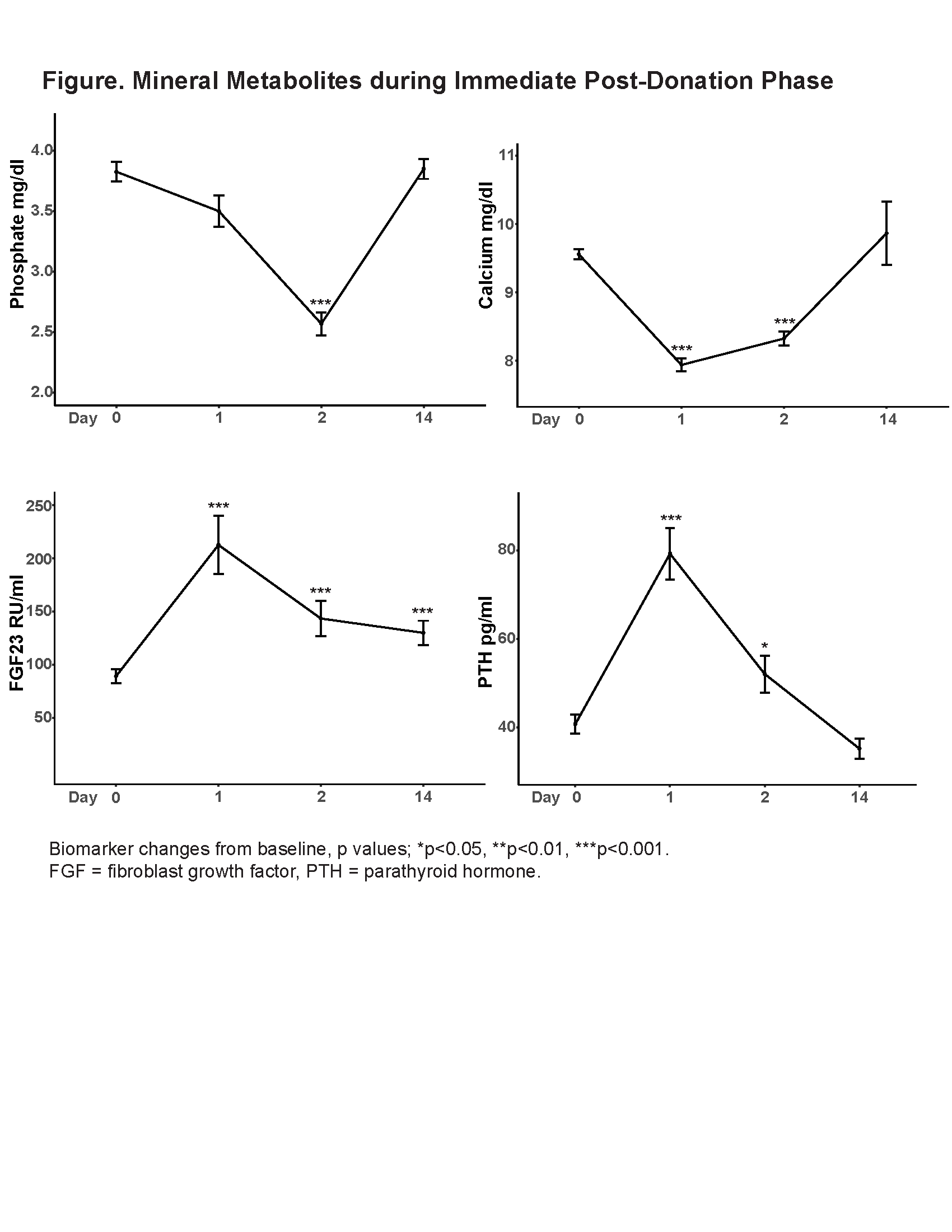
After nephrectomy, estimated GFR decreased immediately from 102.2 ± 17.7 ml/min/1.73m2 to 66.7 ± 15.6 ml/min/1.73m2 on day 1 (p value <0.001). FGF23 and PTH levels peaked on day 1 with 141 ± 55% and 108 ± 38% increase, respectively (both p values <0.001, Figure). Serum calcium dropped to 7.9 ± 0.5 mg/dl on day 1 (p value <0.001). Serum phosphate declined from baseline and reached its lowest point of 2.6 ± 0.5 mg/dl on day 2 (p value <0.001). The serum phosphate nadir on day 2 was significantly associated with log-transformed PTH level on day 1 (p value=0.04), but not with log-transformed FGF23 level on day 1 (p value = 0.66). After 365 days, estimated GFR slowly rebounded to 71.1 ± 17.1 ml/min/1.73m2, but with 30 ± 4% decrease from baseline (p value <0.001). The mean FGF23 levels on day 365 was 103.5 ± 38.8 RU/ml, with significant 19 ± 11 % increase from baseline (p value<0.05).
FGF23 was not significantly associated with serum phosphate decline immediately post-donation, which suggests that acute FGF23 increase following nephrectomy may reflect elevation in C-terminal FGF23 fragments and not the bioactive intact FGF23 hormone. FGF23 increased above normal range 1 year post-donation, suggesting that following up FGF23 levels in this population could be useful for risk prediction of adverse outcomes, including chronic kidney disease progression and development of cardiovascular disease.