Presenting Author:
Benjamin Binder-Markey, P.T.
Principal Investigator:
Julius Dewald, P.T.
Department:
Physical Therapy and Human Movement Sciences
Keywords:
stroke, joint stiffness, hand, fingers, musculoskeletal adaptations
Location:
Ryan Family Atrium, Robert H. Lurie Medical Research Center
C104 - Clinical
Passive finger stiffness changes minimally in chronic hemiparetic stroke
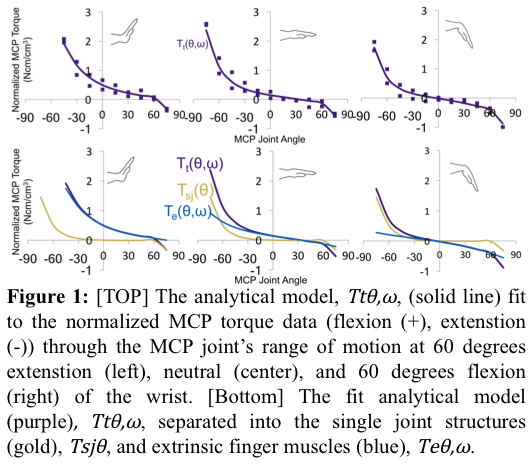
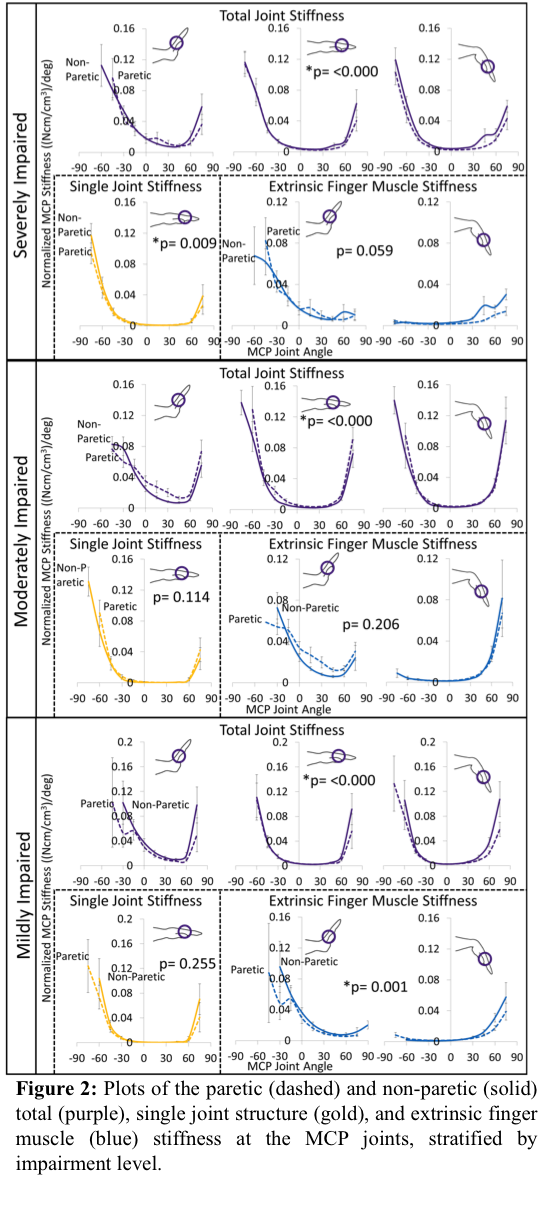
Introduction Hand impairments of individuals with chronic hemiparetic stroke are associated with both neural impairments (weakness, hypertonicity, and loss of independent joint control) and secondary musculoskeletal changes which may result in increased passive joint stiffness of the hand [1]. The neural impairments have been widely studied yet there are limited studies looking into how the stiffness of the hand changes post stroke. Therefore to aid in the timely application of targeted rehabilitation interventions, we aim to determine which musculoskeletal structures contribute to increased stiffness about the fingers post-stroke. Methods Passive torques about the MCP joints were quantified in the paretic and nonparetic hand of 27 subjects (μ=60.4±10.2 yrs old, μ=12.7±7.5 yrs post-stroke). The individuals were stratified by impairment level into those with severe (n=9), moderate (n=9), and mild (n=9) hand impairments. MCP torques were quantified throughout MCP and Wrist range of motion using a custom device, the PIP & DIP joints were splinted. MCP torques were then normalized to forearm volume and EMGs were monitored to ensure the muscles were passive. Torque data for each subject were fit to an exponential analytical model, designed to theoretically separate the torques contributed by the extrinsic finger muscles from other, lumped, single-joint structures (Fig. 1) [2]. Passive stiffness, the derivative of the analytical model, was then used to compare the paretic and non-paretic hands for each impairment level using a linear-mixed model analysis. Results The total normalized MCP joint stiffness was significantly different between the paretic and non-paretic hand across all impairment levels (Fig 2). However, we found the stiffness to be less in severely and mildly impaired hands and modestly greater in the moderately impaired individuals. Yet these overall changes in stiffness across all impairment levels were small. Neither the single joint structures nor extrinsic finger muscles demonstrated consistent changes across impairment levels (Fig 2). Conclusions We found that there were significant changes in total joint stiffness but these changes were small and inconsistent across impairment levels. These results indicate that impairments of the hand in individuals with chronic hemiparetic stroke are not likely related to altered passive stiffness from secondary changes of the musculoskeletal structures. The impairments observed are more likely due to impaired involuntary neural drive and resulting hypertonicity. These finding indicate that future rehabilitation interventions should focus on decreasing the stiffness due to hypertonicity while facilitating voluntary neural motor control. References 1. Kamper, D.G. et al., Muscle Nerve, 2003. 28(3): p. 309-18. 2. Knutson, J.S. et al., J Biomech, 2000. 33(12): p. 1675-81. Acknowledgements AHA Pre-Doc Fellowship: 16PRE30970010; Foundation for PT: PODS II Award; NIH: T32EB009406, 1R01HD084009-01A