Presenting Author:
Principal Investigator:
Department:
Dermatology
Keywords:
aspirin, non-melanoma skin cancer, acetylsalicylic acid, pharmacovigilance
Location:
Ryan Family Atrium, Robert H. Lurie Medical Research Center
C14 - Clinical
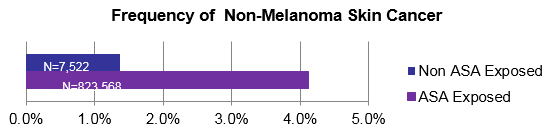
Chronic daily aspirin exposure and association with non-melanoma skin cancer
Background: It is postulated that blocking COX-2 expression may have a chemopreventive role in skin cancer.1 Although COX-2 is not found in normal skin, it is present in actinic keratosis, squamous cell carcinomas (SCC), and in the parenchyma or stroma surrounding basal cell carcinomas (BCC). Moreover ultraviolet radiation is reported to augment COX-2 expression in human skin. Despite anecdotal reports, data on the association of chronic daily aspirin (acetylsalicylic acid, ASA), a COX-1 and COX-2 inhibitor, exposure and subsequent non-melanoma skin cancer (NMSC) has been limited and reports have been somewhat inconsistent regarding such an association. The aim of this study was to determine if an association exists within a large, urban, Midwestern U.S. patient population. Methods: The Northwestern Medicine Enterprise Data Warehouse (NMEDW) is a large, urban, single center electronic medical record (EMR) data repository for > 8 million patients. The NMEDW was searched (Jan. 2001 through Oct. 2015) in order to detect data for all patients age 18-89 who had a follow–up clinic encounter ≥1 year after an index date. Index date for the ASA exposed population was the date of first exposure, while for the control population it was simply the first clinic encounter. ASA-exposed patients had ≥ 1 year of ASA 81-325 mg daily dose (N=7,522), while the control population had no ASA exposure (N=823,568). NMSC diagnoses were detected by the International Classification of Disease (ICD) code for NMSC (ICD-9: 173.0-173.9) and were included only if the diagnosis occurred ≥ to 6 months after the index date. Patients with a history of NMSC prior to the index date were excluded from analyses. Data included age, race, and gender. Adjusted Odds Ratio (OR) for NMSC with ASA exposure was determined by logistic regression analysis with 95% CI. Results: A total of 831,090 patients met inclusion criteria for this study and after adjusting for age, gender, and race, a significant association for NMSC subsequent to daily exposure was determined (OR: 1.57; 95% CI 1.4-1.76). 7,522 patients had daily ASA exposure, of which 310 had a subsequent diagnosis of NMSC. 823,568 controls without ASA exposure had 11,284 subsequent NMSC diagnoses. The frequency of NMSC in the exposed population was more than twice that of the non-exposed population. Discussion: A meta-analysis reported a reduced risk of NMSC with daily ASA use2, another reported a reduced risk of SCC with ASA use of borderline statistical significance3, and another reported no statistically significant chemopreventive effect of ASA4. Our retrospective study found an increased frequency of NMSC subsequent to chronic ASA exposure which may be explained by a difference in study design. Further exploration of this association is warranted to more clearly establish the role of chronic aspirin exposure and subsequent diagnosis for NMSC.